

I just got a third dose of MMR vaccine. Here's why.

About a year ago, I wrote a detailed piece about measles infection and disease focused on the myths about its severity and nonexistent health benefits. There, I did express that 2 doses of MMR would in theory be enough for basically everyone to maintain lifelong protection, but I did give some caveats, noting that the currently circulating genotypes of measles were more of a problem for antibodies than older ones. When I wrote that piece, I did not imagine that public health would be in the grievously imperiled state it is in today. But, circumstances change and you have to adapt.
A note: in this post, I mainly discuss my individual-level considerations rather than public health considerations. This should not be taken to mean that I believe that individual-level considerations are more important than public health considerations. They both have a key place in vaccination decisions and often are not in conflict.
My considerations

When measles outbreaks occur, it is very alarming not just because of the fact of measles itself, but rather because of what they portend. Because of its exceptional contagiousness1, measles tends to be the first vaccine-preventable disease that shows up when vaccination rates drop- but it is typically followed by others, such as pertussis. Given the current situation in the US Southwest with measles outbreaks, this is a very concerning sign. Because of measles’ effects on the immune system, it is a threat to herd immunity against other pathogens as well. Some experts have gone as far as to suggest that a measles infection warrants redoing the entire vaccination schedule because of this, though there is no official recommendation for this. Data from the UK also suggests that waning of measles immunity from the vaccine may contribute to outbreaks, though that waning is still very slow (0.039 % per year of age), largely because of a lack of regular exposures to boost immunity to measles, but this is still thought to be enough to contribute to outbreaks given gaps in immunization coverage.
Still, I have perhaps given you a red herring. You see, measles is not the primary driver for my motivation to get a third dose. The actual one is: mumps. As I have already discussed measles in depth here, it is worth summarizing a bit about mumps, which I have done in this footnote2.

You may have heard that the US has consistently had mumps outbreaks, usually in colleges, despite the fact that the MMR vaccine has reduced the incidence of mumps by >99%. There’s a reason for this, and it was recently well-articulated by vaccinology hero Stanley Plotkin:
The reason for [the waning protection of mumps vaccines] is quite simple and has been known for years: namely that the Jeryl Lynn strain carries an HN protein of genotype A, whereas circulating mumps viruses carry a genetic component that is different, namely an HN protein belonging to genotype G.4–6 Inasmuch as the HN protein induces neutralizing antibodies, it is not surprising that a difference between that protein in the vaccine and in circulating mumps virus changes the vaccine’s ability to protect. In that circumstance, more antibodies to the HN protein are needed to neutralize a type G mumps strain than a type A strain.

Even more recently, a study was conducted examining the ability of a mumps HN protein vaccine to induce protective immune responses in animals. Plotkin’s position is the necessity of a new mumps vaccine which would induce more robust immunity to the G genotype, but he does float the idea of a third dose of MMR before people go off to college, though noting this would be difficult to enforce for people who don’t go to college (on this point though, I think in saner times it would have been enough to do that given that college campuses are the major sites of outbreaks as it is). Previous work has found that a third dose of MMR is safe (though the sample size here is limited3) and appears to be effective, and as it is, a third dose of MMR is frequently used to control mumps outbreaks, and there’s even a CDC guideline to do so. Given these facts, worsening measles outbreaks throughout the US, and an administration doing all it can to sabotage vaccination programs, this was a no-brainer for me.
For completeness, I did consider rubella as well in my analysis- but it was a minor factor. A summary of rubella from me can be found in this footnote4. The major risk from rubella is to fetuses, and while it can rarely be serious in adults (for example, causing myocarditis), a single dose of rubella vaccine is generally enough for lifelong immunity for most people, and in outbreaks of rubella the vaccine has been measured to be extremely effective (99.5% against disease in one well-documented example), but does not provide “sterilizing” protection (meaning it cannot prevent infection altogether- in one outbreak, evidence of reinfection was seen in 50% of vaccinees, yet no one became sickened with rubella). The estimated rate of seroreversion (loss of detectable rubella antibodies) is 0.012% per year. Because I am not capable of becoming pregnant, the risk of rubella was not especially salient for my decision, though, in hindsight, given the questions about accessibility to rubella vaccines, it may be prudent from the lens of indirect protection regardless.
Why I didn’t bother checking my titers
It’s commonly suggested that people check antibody titers to vaccine-preventable diseases before getting a booster. This is not an unreasonable suggestion- but I didn’t feel it was worthwhile in my case. Titers are useful when definitive evidence of immunity is needed, such as healthcare workers and their immunity to hepatitis B virus or when someone who is trying to conceive has their rubella and varicella titers checked. But as tests, they are imperfect (as all tests are).
Many of the vaccine-preventable diseases lack an established absolute correlate (a threshold measure for protection) for an antibody titer that can be used to infer protection (or lack thereof). This is the case for mumps, for example.
Even in cases where there is some kind of absolute correlate, there can be issues when generalizing to strains other than those from which the test antigen is derived (e.g., measles genotypes D8 and B3 are less susceptible to neutralization by antibodies elicited from the A genotype in the vaccine), and variation in exposure conditions can also play a significant role (i.e., the inoculum size).
While not the case for measles, mumps, or rubella, protection from a few vaccine-preventable diseases (notably shingles) does not appear to depend much on antibodies at all, but rather on T cell responses, which titers cannot inform.
Commercially available antibody titer tests generally work by an ELISA or ELISA-like assay, which can identify binding but cannot access the functional activity of antibodies, like neutralization, which are the major correlates of protection for some diseases (e.g., measles has an absolute correlate of 120 mIU/mL on a microneutralization test- which requires using your antibodies to see whether they actually block measles infection).
There is a nontrivial false negative rate for the titer assays depending on the specific vaccine-preventable disease (e.g., some can be controlled by memory B cell responses, but, over time, titers might decline to subprotective levels). If this occurs, the conclusion will be to just get a booster regardless.
Given these factors, I figured it made more sense to just go get a booster than bother getting poked an extra time and going through the wait for results. Plus, titers would not have been informative about the risks relevant to me anyway.
There will be roughly 12-18 new cases for every case of measles on average in a population without pre-existing immunity- though in individual outbreaks values in the range of hundreds and even thousands have been documented. There are multiple factors contributing to the extraordinary contagiousness of measles. First, the period of infectiousness is long- 4 days before to 4 days after the rash, and the rash usually lasts 5-6 days, meaning 14-15 days of infectiousness. Note that measles becomes infectious before the appearance of the rash, and in some cases, before a person even has any symptoms. Another factor is the nature of spread- measles aerosols can remain suspended in the air for many hours. This means that if someone infected with measles so much as passes through a space with other people, that space is now an exposure risk for long after the measles-infected individual leaves.
Mumps virus infects through the upper airway and predominantly replicates therein, before eventually getting into the blood and going everywhere.
The virus has multiple receptors, which are (in aggregate) ubiquitous throughout the human body body (GM2 ganglioside, α-2,3-linked sialic acid-containing trisaccharides, and sialyl Lewis x), meaning the virus can infect almost any human cell. It does preferentially infect cells of the central nervous system and glandular tissues.
The major sign that mumps is known for (and where it gets its name) is the massive swelling of the salivary glands (parotitis) induced by mumps; about 5% of mumps cases will not have parotitis. Note that parotitis and mumps are not synonymous, as multiple other infections can cause parotitis.
Mumps can also be a cause of viral meningitis, as the virus can penetrate into the brain through the circumventricular organs, at a frequency of 1-10% of cases. If the virus starts an infection of the brain itself (encephalitis, 0.1% of cases), there is a 1.5% risk of death.
Mumps is also threatening for fertility, particularly if contracted after puberty, as it can cause epididymoorchitis (inflammation of the testicles and epididymis) in males and (less commonly- ~5% of adult females) oophoritis (inflammation of the ovaries) in females. Epididymoorchitis is the most common complication of mumps, occurring in roughly 15-30% of adult males, and can result in loss of fertility and possibly endocrine disruption of testicular function, though the absolute risk is thought to be low, even if both testicles are affected (though this is rarer at 17% to 38% of cases of epididymoorchitis). Oophoritis also rarely results in frank infertility. If epididymoorchitis develops, the pain can persist for weeks after apparent recovery. Mumps RNA can also be found in semen as late as 40 days after infection, and in at least one case has been associated with the development of anti-sperm antibodies, which likely have long-term harms to fertility.
Mumps has also been suggested to be able to cause early pregnancy loss, though not all evidence on this point is consistent. If infected in pregnancy, mumps can also cause mastitis (inflamed breast tissue), and mumps has been isolated from human breast milk after infections.
Mumps can also cause pancreatitis (about 3% of cases based on a retrospective survey), which in rare cases can be quite severe; children with pancreatitis usually report belly (epigastric) pain and tenderness, fever, chills, vomiting, and prostration. Relatedly, there is a long association between mumps infection and the onset of diabetes.
In rare cases, mumps can also attack the kidneys. Most of the time, this does not result in permanent damage, but it can manifest as fulminant glomerulonephritis which can be fatal. Mumps also frequently causes some hearing loss, and rarely can result in complete deafness- this can be seen even in asymptomatic patients.
Uncomplicated mumps is managed with conservative treatment. Nausea and vomiting are common but rarely require intravenous fluids. Acidic foods may be difficult to tolerate. Pain management for orchitis may warrant codeine or meperidine; otherwise aspirin, NSAIDs, and acetaminophen are adequate for parotitis. There is no specific antiviral therapy for mumps, but systemic interferon α2 (IFN-α2) has shown an effect in a pair of small studies for restoring normospermia and resolving symptoms in mumps orchitis. If infection of the central nervous system occurs, patients have reported relief after lumbar puncture (spinal tap).
Mainly in adult women who do not have evidence of immunity to rubella, temporary joint pains may occur with MMR vaccine.
Rubella is spread through the air when people inhale the rubella virus and by direct contact.
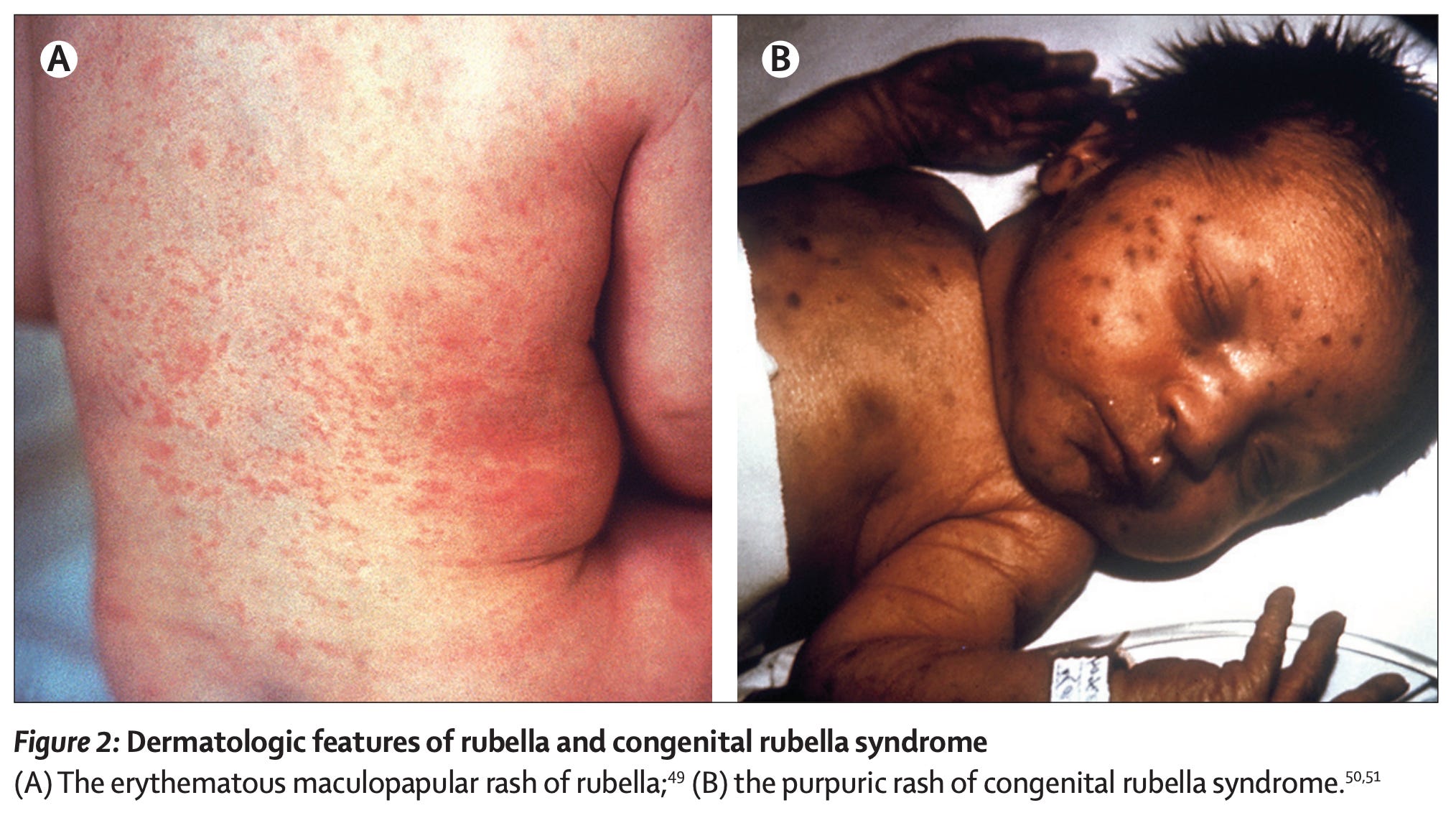
It is a generally mild disease in most people (asymptomatic in a quarter to half of people), only rarely causing severe illness and usually just appearing as a rash with nonspecific flu-like symptoms and a low-grade fever (this is sometimes called acquired rubella or postnatal rubella to distinguish it from congenital rubella).
However, rubella can have catastrophic, lifelong consequences if contracted in pregnancy, particularly in the first trimester, because it can infect the fetus. This can cause a condition in the fetus called congenital rubella syndrome (CRS). If CRS occurs, about 20% of first-trimester cases will cause miscarriage or stillbirth. Of those that survive, 85% will have congenital anomalies (although in some cases the abnormalities become apparent only later in life), but this risk declines the later in pregnancy the infection occurs. The most well known of these are blindness, hearing impairment (including deafness), and congenital heart defects, but the harms are far more extensive with neurological defects (intellectual disability, microcephaly- a condition in which the head is abnormally small because of a problem with brain development), low birth weight, diabetes, immunodeficiency, and potentially even progressive panencephalitis (a type of brain infection by the rubella virus), which is fatal and occurs in the second decade of life. In essence, CRS can affect every organ system. These disease manifestations are believed to be fundamentally because the immune system never clears the virus after the initial infection in utero and so there is a persistent immune response against it that damages our tissues (rubella virus can be isolated years, even decades after the in utero infection from individuals who have CRS).
It has also been noted that human stem cells do not differentiate into more specialized cells as well upon infection with rubella virus, and to combat the infection, cells may commit suicide (apoptosis), which helps to explain why so many developmental problems occur.
Because rubella is so dangerous if contracted in pregnancy, it is critical to be up to date on rubella vaccination. Still, rubella vaccines (MMR) should not be given during pregnancy because there is a theoretical risk of the vaccine strain virus infecting the fetus.
However, in studies where rubella vaccines were inadvertently given to pregnant individuals, no cases of congenital rubella syndrome were observed out of hundreds of individuals, so if a rubella vaccine is accidentally given during pregnancy, it should NOT be taken as reason to terminate the pregnancy. I am aware of a single case of congenital rubella syndrome arising from the vaccine in all of its history, which is noted in this report to be the first documented case as of 2023.
Because of these factors, individuals who hope to become pregnant should receive rubella vaccines at least 4 weeks before actually becoming pregnant. Clinical guidelines for obstetricians call for screening individuals of childbearing potential for immunity to rubella annually (as well as measles, mumps, rubella, hepatitis B, varicella, tetanus, diphtheria, and pertussis).
There are no specific treatments for rubella. Postnatal rubella is generally mild and so the only treatment is management of symptoms until the illness naturally resolves. In the event that an individual who does not demonstrate immunity (i.e. antibody titer) against rubella is exposed, there are no specific antiviral medications that can be offered. Some experts have argued for the use of immunoglobulin in such circumstances, but the benefit is not clear.
In the past, when rubella was common, it would typically be considered grounds for abortion if infection occurred in pregnancy. Infants born with CRS are contagious and are considered contagious until they have two negative viral cultures at least 1 month apart after they reach 3 months of age. They can remain contagious for over 1 year. Otherwise, the manifestations of CRS are managed largely in the same way as if they were from any other cause. Congenital heart defects should generally be repaired surgically if they cause a problem. Children with immunodeficiency may require antibody replacement therapy for the rest of their lives. Children with deafness should undergo thorough evaluation and be enrolled in training programs to help manage their disability. Problems with vision should be addressed by an ophthalmologist.
Thank You:
This is some of the most important health Information that I believe anyone can ever learn.
The Information presented in this article should be mainstream knowledge and should receive regular media attention, it is a tragedy that the dangers of all three viruses: Measles, Mumps and Rubella are not widely known. Also, it is apparent that the M.M.R. vaccine is one of our most important Immunizations.
Also, with the understanding that we need a new Mumps vaccine, vaccine science and research (an already neglected and not nearly enough a societal priority), may be even less prioritized in the coming years?
With the prevalence of immune modifying drugs increasing, the option for a booster requires stopping those drugs: perhaps better studies there could inform which ones actually present a risk as it isn’t likely ALL of them.
I have other physician friends who get tested and revaccinated due to only brief seroconversion on testing. We suspect they likely have adequate immunity, to your point.
I feel like a routine third dose for college students has been floated for so long but never has materialized.
Personally, I think given the uptick in outbreaks, perhaps more details on who, how long from the complete series, and of course more stringent requirements… not happening soon.