

Some Hantavirus Updates: Focus on Misperceptions and Miscalibrations
Current as of May 7, 2026 2:30 PM EST.

Since my last post, it seems that there is a huge response on social media with many people understandably anxious regarding the possibility of Andes virus (hantavirus) becoming a pandemic. We are very far from that being a justified concern by the evidence from this current outbreak, and I want to spend some time explaining why while also including some important updates on the situation.
Before I go into this, I want to do two things.
First, I want to address the anxious people directly: I get it. I was there in 2020 as well. I lived through it too. I saw SARS-CoV-2 defy expectations over and over and there were instances where we were too slow to move in an evolving situation. Nevertheless, we have to stick to the facts that we have and adjust as we learn more. We don’t get useful action out of panic. What we do know about Andes virus, as it pertains to global risk, is reassuring. Until evidence saying otherwise emerges, those are the facts on the ground.
Second, I want to share the WHO’s recent Live where they took questions about the situation because I think people will find it to be helpful and informative:
I did use information in this media briefing to help with the content on this post.
What does it take to contract Andes virus?
Is Andes virus airborne?
In the broadest terms, Andes virus can be contracted by inhalation of an infected long-tailed colilargo’s urine, feces, or saliva. How it spreads from person-to-person is less well established, but it is also probably from inhalation of infectious viral particles. That has led some people on social media to argue that this means the virus is airborne1 and thus we’re going to relive January 2020 with COVID-19 all over again. We’re not. Just because an infection is contracted by inhalation does not mean it is easy to contract. Yes, we all breathe—we can’t avoid that—but saying that the virus is airborne is not a complete description of how it spreads.
Previous outbreaks have shown us specifically that to spread, the virus has needed prolonged, close contact with someone who is symptomatic, particularly while they have a fever. This does not contradict that the virus is spread by inhalation. In the 2018 outbreak in Chubut Province, Argentina, there were 82 healthcare workers exposed to symptomatic patients, 45 of whom were in the ICU, only a few of whom used any personal protective equipment while in direct contact with a patient and none of these individuals contracted Andes virus as far as we can tell (but there were 2 events of hospital-acquired Andes virus where 3 people contracted it in this outbreak, but none were healthcare personnel). While there are many potential reasons for this, I hesitate to speculate on the virological aspects that could explain this. The relevant point nonetheless remains: transmission required close, prolonged contact with someone symptomatic. To date, there is no clear evidence of human-to-human transmission of Andes virus occurring before a person is symptomatic or from asymptomatically infected individuals. That doesn’t mean that it couldn’t ever happen, but we have known about Andes virus since 1995 and we have documented about 3000 human cases, with the vast majority not being the result of human-to-human transmission. With a condition as dramatic as hantavirus pulmonary syndrome, it would be hard to miss insidious spread from asymptomatic/presymptomatic individuals.
Is Andes virus behaving differently from how we would expect?
I would argue that it isn’t, caveated on the point that this is an outbreak occurring on a cruise ship. That particular event—a hantavirus outbreak on a cruise ship—is unprecedented but the context is informative. Adam Kucharski recently shared the figure below from this paper, noting that “Passengers had median of 20 (IQR 10–36) unique close contacts per day, and over 60% of contact episodes were in dining or sports areas.”
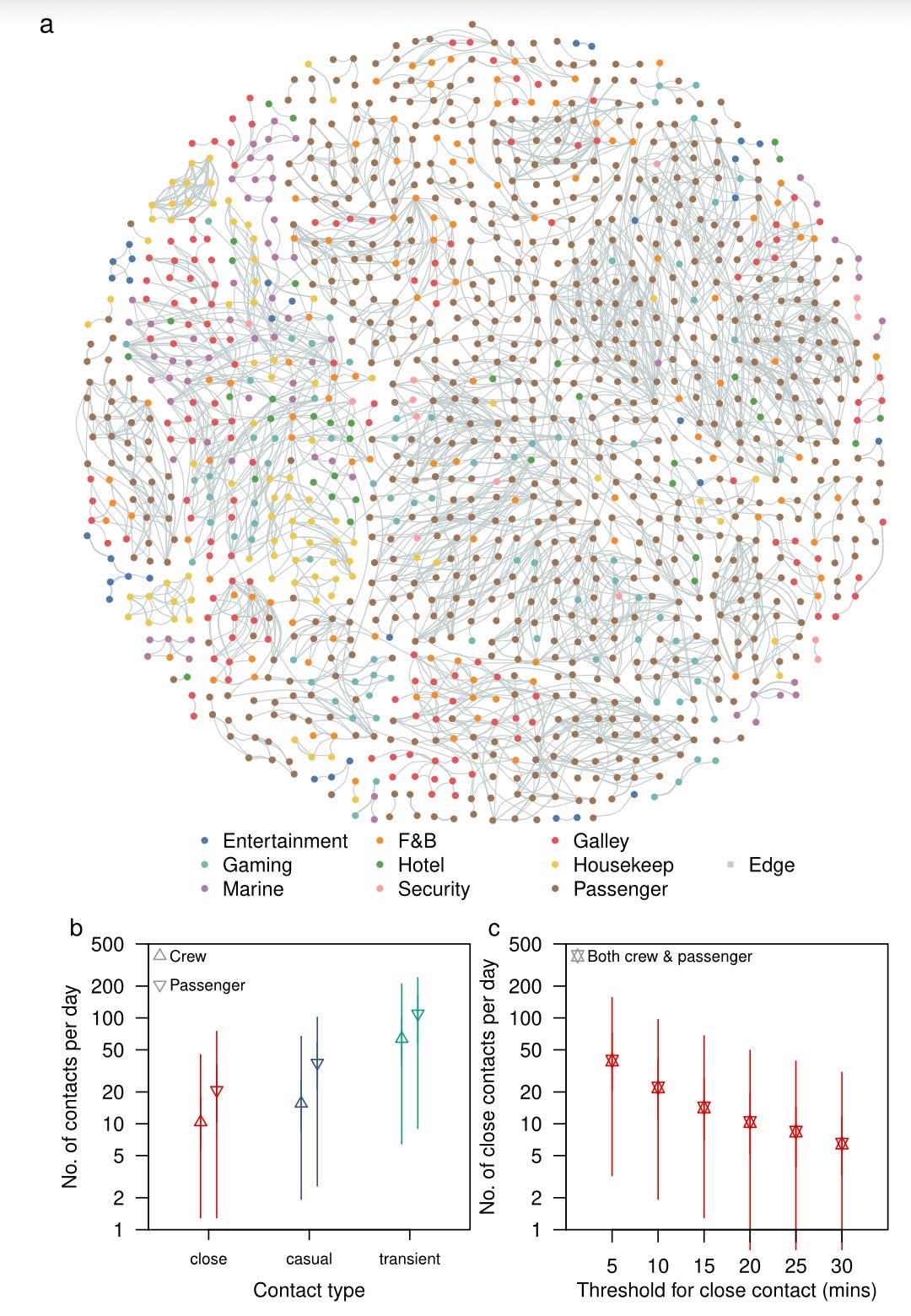
That is an extraordinary opportunity for any infectious disease to spread, and we have seen it time and again with norovirus, influenza, and COVID-19 on cruise ships. So far, outbreak investigation has not reported a case of someone on the MV Hondius who contracted the infection in association with brief, casual contact. The conditions for Andes virus to be able to spread are being met on the cruise ship. That doesn’t mean that they are easy to meet outside of it.
Now, it is not impossible that the Andes virus in this outbreak could evolve to spread more efficiently between people during this outbreak and we may be surprised, but the weight of past experience with it does not support that idea and acting as though it has already happened serves no one.
Virus RNA and Infectious Virus
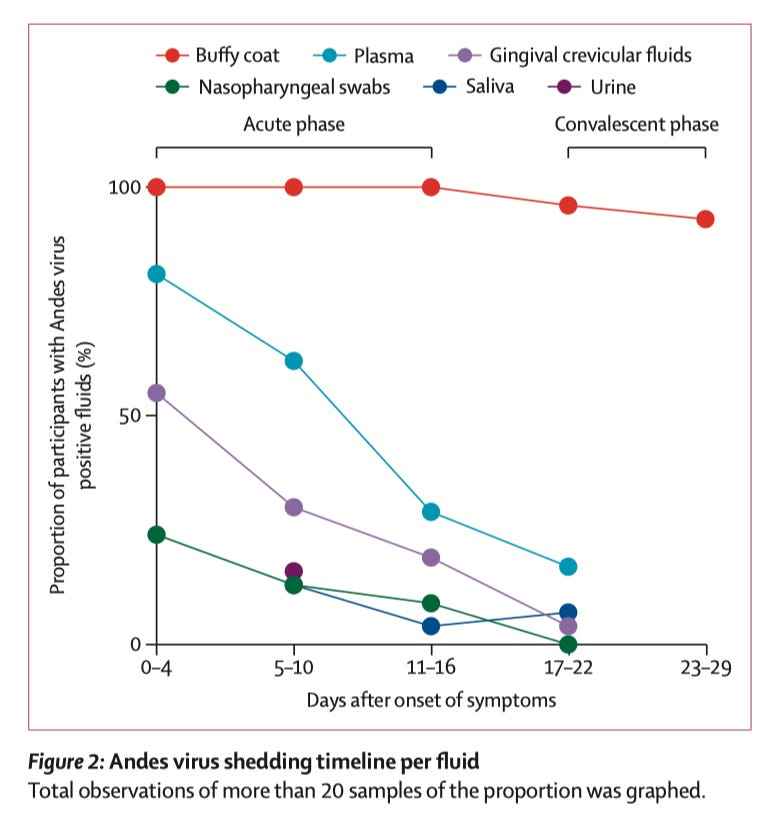
This is a point that has caused much confusion from the COVID-19 pandemic and it remains a point of confusion in this Andes virus outbreak. Fortunately, we have data. First though, a bit on the principle: virus RNA in a given site cannot be presumed to equal actual, replication-competent virus without additional testing. We actually have a great study addressing exactly this. In this study, 131 individuals with confirmed Andes virus infections provided saliva, gingival crevicular fluid, plasma, nasopharyngeal swabs, and urine on days 0, 7, and 14 after hospitalization, with surviving patients consenting to follow-up. Here is the trend in viral RNA:
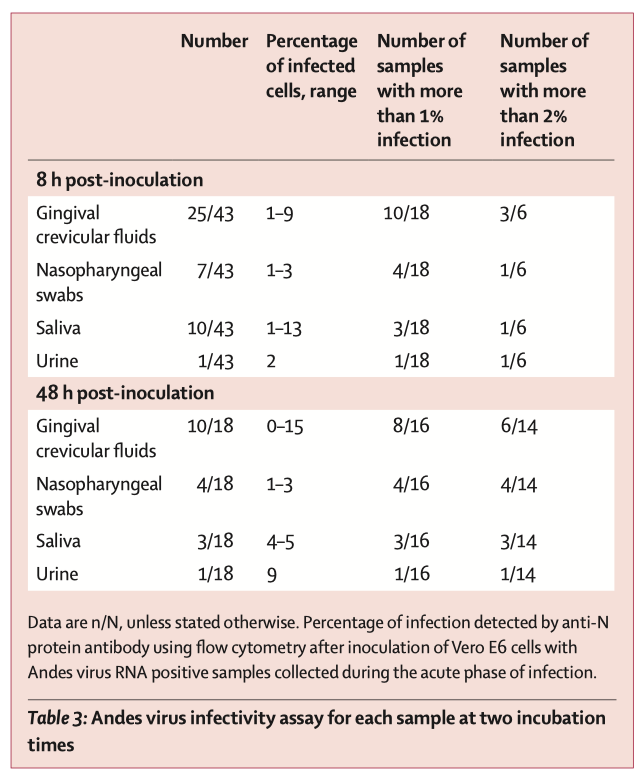
But the team did a really smart thing next: they tested to see whether samples from acutely ill patients were infectious in Vero cells. Here’s what that looked like:
We know that it can take a long time for RNA from Andes virus to clear. This is especially true for immunoprivileged sites (e.g., one survivor had detectable viral RNA in his2 semen for 71 months—virus could not be isolated from any sample during that period by culture).
Andes virus cases off the boat? Not exactly and not yet.
It was recently reported that a French national on the flight from St. Helena to Johannesburg taken by a woman from the MV Hondius who died of Andes virus shortly thereafter has developed symptoms, as has a flight attendant (though it is unclear whether she was on the same flight and that information is not being released for privacy reasons). It is way too soon to declare that this means that Andes virus has begun to spread to people not on the MV Hondius cruise ship. Here is why:
We do not know what symptoms they have.
The initial symptoms of Andes virus infection are extremely nonspecific flu-like symptoms.
Andes virus has a long incubation period relative to many other microbes that can cause flu-like symptoms.
Current reports do not provide detail about the symptoms either the flight attendant or the French national are experiencing beyond saying that the French national had respiratory symptoms. Still, at this stage, it is not likely that either of them have full-blown hantavirus pulmonary syndrome just because of the timing. As a reminder, Andes virus has an incubation period (the time it takes from the onset of infection to the onset of symptoms) of 1-6 weeks (some sources say up to 8 weeks) and, in most cases, 2-3 weeks. The flight in question occurred on April 25, 2026. That’s a bit less than 2 weeks ago. It’s within the incubation period so it can’t be ruled out that this isn’t hantavirus, and from a public health perspective, the appropriate response is to treat it as though it is hantavirus until proven otherwise and move these patients into isolation while tracing their contacts and awaiting test results.
However, here are some representative incubation periods from other pathogens that can cause flu-like illness:
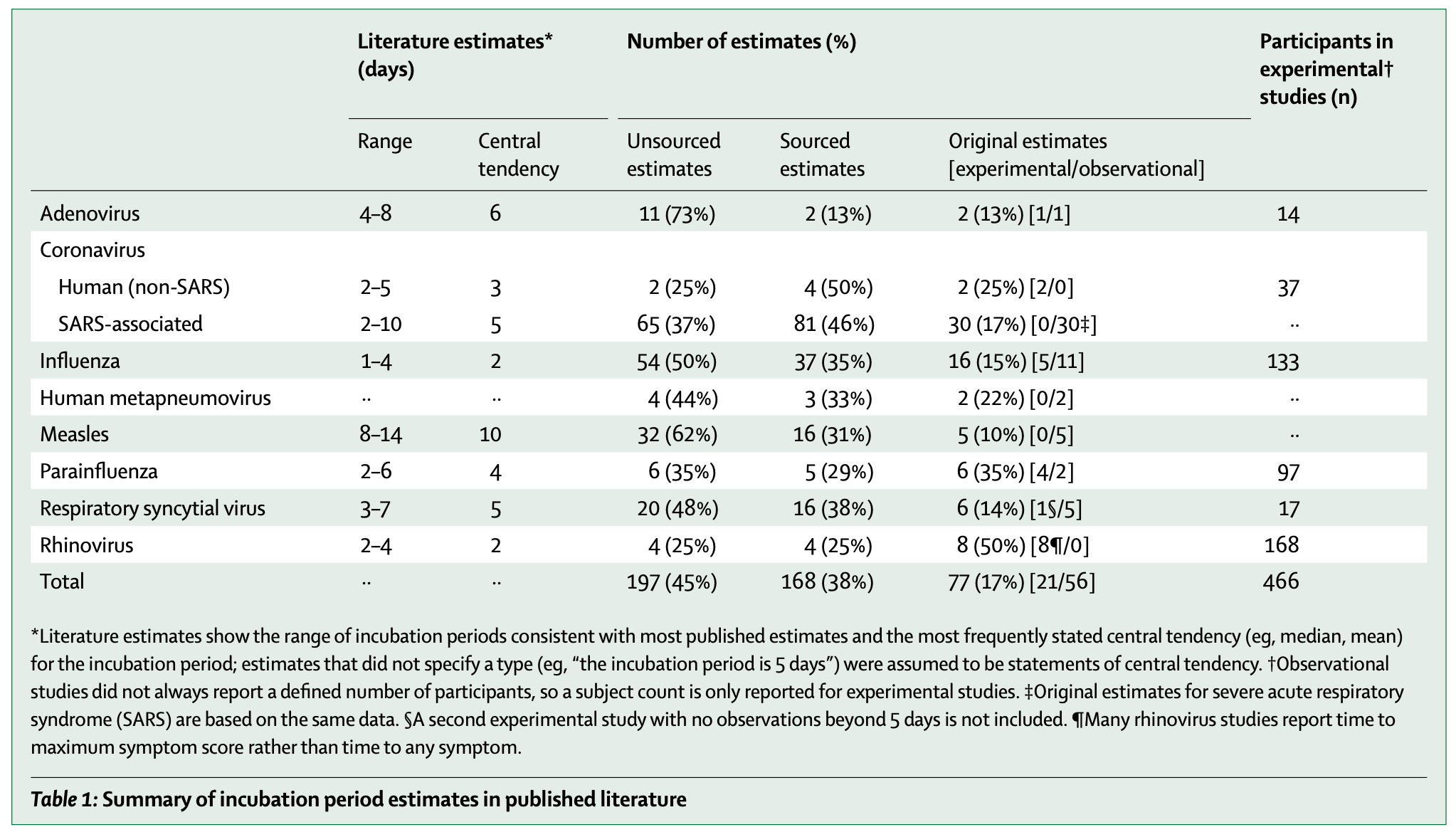
Most of these are quite common respiratory viruses (SARS-CoV-1 is a notable exception) and they have MUCH shorter incubation periods than Andes virus and they are known to infect people with much greater facility than Andes virus.
Now, I want to be clear that I am not saying that there is no possibility of onward transmission of Andes virus on that flight or that we won’t find cases of Andes virus connected to the cruise ship but in people not on the cruise ship. In an outbreak response, you uncover things and we should expect to see more cases over time if only because we are looking for them. But as of the time of writing this, all cases of Andes virus (either suspected or confirmed) are in people who traveled on the MV Hondius.
What should I actually do to protect myself against hantaviruses?
I think that there are much more immediate infectious threats that merit concern and are much greater risk than Andes virus for most people reading this (i.e., everyone who is not on the MV Hondius, although even that’s debatable). For example, we are heading into summer and that almost certainly means we’re going to have another wave of COVID-19. If you are worried about exposure to hantaviruses, you should bear in mind that the main source of infection is not other people, but rather rodents. If you live in close proximity to rodents, it is important to take time to familiarize yourself with how to properly clean up after them. Additionally, hantavirus vaccines are still needed so it’s worth considering participation in clinical trials to study them.
Please remember: we have had Andes virus outbreaks in the past and we have successfully contained them. We need to have patience and ensure that we are thoughtful in how we engage with emerging information, i.e., doing our due diligence to confirm it and not spreading unverified rumors.
I’ve also seen some confusion still regarding the meaning of airborne vs. droplet. Both of these refer to specific transmission precautions that need to be taken with a given pathogen, rather than distinct routes of transmission. It was long thought that we could dichotomize spread of respiratory pathogens into those that were transmitted via fine aerosols with prolonged hang-times like measles or tuberculosis, and those spread via large droplets that, while inhalable, typically fell to the ground quickly and had less opportunity to infect. As the COVID-19 pandemic has shown us, this dichotomy is misleading and does not reflect the realities of spread, so in this post, I do not distinguish between them and I describe pathogens that can be contracted this way as those you can get via inhalation.
I assume that the individual uses male pronouns, but I may be mistaken.
While vaccines for prevention of many viral illnesses are a significant benefit for the public health, there remains a critical need for therapeutics that are capable of addressing host targets and not simply searching for new antivirals, new monoclonal antibodies, IL-6 inhibitors and “hammer-style” steroids to suppress the host response. They all require vast resources and immune escape is the norm when science fails to address critical targets. There are candidates in the repurposed “cabinet” that have great potential and decades of safety data as well.
Not to be spreading misinformation but some may recognize that rodents as a class of animals are very diverse. Wiki notes:
Mice House mouse, field mouse
Rats Brown rat, black rat
Beavers North American beaver
Hamsters Syrian hamster, dwarf hamster
Guinea Pigs American guinea pig, Peruvian guinea pig
Chipmunks Eastern chipmunk, Siberian chipmunk
Prairie Dogs Black-tailed prairie dog, white-tailed prairie dog
Marmots Groundhog, yellow-bellied marmot
Rodent Characteristics
Rodents are characterized by their continuously growing incisors, which require constant gnawing to keep them from overgrowing.
They are found in a variety of habitats, including forests, grasslands, and urban areas.
Rodents make up about 40% of all mammal species worldwide, with approximately 2,360 species identified.